Traffic Shaping and Bandwidth Management For Novell NetWare
A progressive, degenerative disease of the cornea.
Hi,
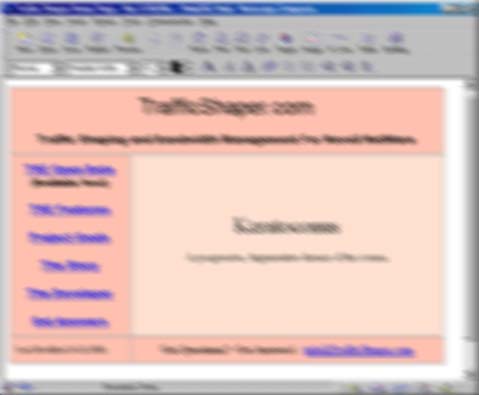
I am afflicted with a relatively rare cornea disease called Keratoconus aka KC. With the KC in my left eye, the above graphic illustrates what I can see unaided from a distance of about 18". Some people find it difficult to look at this image for even a few seconds - as it causes severe eyestrain an headaches. Welcome to the life of those with KC. Below you will find some of my favorite links to KC resources. I encourage you to learn more about KC. If you happen to have butt loads of money please donate to one of the KC research funds.
About KC
Basically, Keratoconus is a disease which thins the central region of the cornea. This results in a deformation of the curvature of the cornea, often leading to corneal scarring, and a subsequent loss of visual acuity. It causes a multi-focal astigmatism which is not easily corrected by glasses, if at all. Typically rigid contact lenses are required to restore vision. Unfortunately, due to the irregular shape of the cornea and possibly due to an underlying histological mechanism, these contact lenses are not well tolerated in many cases - resulting in only a few hours a day of relatively decent vision.

In some cases, even contact lenses cannot correct the vision or cannot be worn for a sufficient number of hours. A corneal transplant is then necessary to restore vision. While KC is typically not a cause of blindness - it is the leading cause for corneal transplant surgery. This surgery, as you can imagine, is not without its problems. Other treatments for KC, such as "intacts," a small glorified rigid gas perm lens surgically implanted into the cornea, offer some hope for treatment in the future.
![]()
( If the eye offends thee... Ouch! )
Only about one in two thousand are afflicted with KC. KC is also associated with several genetic diseases, such as Marfan syndrome, and other genetic disorders which impact the connective tissues. The cornea itself is a very unique tissue as it does not have a blood supply and relies on secretions to obtain oxygen and nourishment. This is very similar to other tissues, such as tendons and cartilage, which lack a blood supply. About half of those with KC have some other disorder which predisposes them.
KC and Me
I was diagnosed about 6 years ago, in my late 20's, but I was probably pre-keratoconic for some time. I have relatively mild-moderate KC in my left eye and have started to see a slow degradation in my right eye, which is still considered pre-KC. Strangely enough both eyes followed the same progression. About 6 months prior to noticing a decrease in vision in my left eye, I would wake up in the middle of the night with a stabbing pain in my eye - as though a grain of sand were squarely placed on my cornea. I used bottle after bottle of eye wash, went to the eye doctor several times, and so on and nothing was found that could be the source of the pain. It was written off as being something spurious. After a month, the pains went away and never returned.
( After dealing for 3 years with the wrong eye doctors, I finally
stumbled on a real expert who immediately hit on the problem: a reoccuring
corneal erosion, which I have been able to successfully treat. It
is possible this is part of the KC progression in that they can be caused
by newly forming patches of endothelial cells groaning on the cornea due
to small tears caused by the progression of the disease. Or is could
be the other way around: the corneal erosions served as a chronic insult
to the cornea ( i.e. a cause of KC akin to the mostly discredited "eye rubbing"
theory. Lesson: find an expert in KC, not someone who knows how to
spell "KC." )
Of course my vision had started to deteriorate in that eye to the point where I could not read type a foot away with my glasses. It was not due to a change in prescription - i.e. "power" of the lenses, but rather a lumpy distortion in the cornea which gives the effect of trying to read through a translucent shower curtain or that ripple glass. I have since had the same pains in my right eye and have noticed the same deterioration in vision. An expert explained that as the cornea thins, the stresses increase in the central region possibly causing the fine network of nerves there to be stretched, causing phantom pain. It is also possible that the stretching caused the formation of a corneal erosion which caused the pain. Eventually the stretching stops or the nerves in question finally "give up" on trying to signal the pain, or the erosions heal.
I got to the point where I was getting about 2 hours of "good" vision a day before the contacts bother me to the point of removal. Some days I could not keep them in at all. This is relatively poor tolerance of the contacts. I also have dry eye for which I was taking cyclosporine eye drops. These seemed to help. However what has really improved things is fish oil pills, daily eyelid cleaning ( yes, eyelid cleaning ), and hypertoniciy ointment. I'm no natural health nut, but the fish oil worked for me and provide numerous other well document benefits.
Nerves in the cornea detect when the eye is in need of tears, when irritated, and trigger tear production. When the eye is chronically irritated, the tear producing glands essentially become exhausted which in turn causes a self sustaining inflammatory reaction which turns off tear production. Having a piece of plastic in your eye and having the nerves in your cornea being stretched tends to do that!!! Ouch! The Cyclosporine is a powerful immunisupressant - in fact it was the original anti rejection drug which paved the way for transplant surgery. By suppressing the self perpetuating immune reaction, normal tear production can be restored, reducing inflammation and increasing contact wearability. Or at least that is the theory. Frankly, I'm less impressed by cyclosporine drops compared to the fish oil results.
Obviously talk to your doctor! Duh! The EPA and DHA in fish oil has been show to interfere or shift the balance of prostaglandin production to suppress inflammation. This is obviously NOT something you wan if you are not otherwise healthy. Again see your doctor before attempting self medication. When shopping for fish oil read the ingredients and look for the highest concentration of EPA and DHA delivered per pill. Flax oil contains ALA, which some people can convert to EPA and DHA. However many people cannot, and many others convert this so inefficiently the flax oil is essentially useless for this purpose. ( There is a lot of evidence, however, that ALA alters lipid metabolism favorably, improves glucose regulation, and helps in weight loss. ) My current net intake of 1000 mg EPA, 400 mg DHA, 4000 mg ALA daily - spread throughout the day. Note that the dose indicated here will may cause "thinning" of the blood and an increase in clotting time. However, my "dry eye" symptoms have improved with fish oil.
I currently use a dual lens system consisting of RPG and the latest 30-day continuous wear soft lenses. I can get >10 hours a day of wear out of this practical and relatively inexpensive system. This is a vast improvement over the 2 hours a day I had prior. There is, however, a tradeoff in terms of vision. With each transition from one material to another, you end up with additional distortion and reflection which reduces visual acuity.
KC Misconceptions
Many people ask all sorts of irritating questions about KC ( which you can avoid by visiting the following sites ) and that I have to suffer each time I talk about it. So here is my mini-FAQ on KC so I won't have to hurt you!
You use a computer a lot... is that what is making you go blind?
Yes, I do use a computer a lot. But I am by no means "going blind" because of it. Watching a computer screen has been shown to decrease the blink rate in people. This can cause a reduction in the number of times tears are wiped over the surface of the eye - leading to eye dryness. The over the counter drops - or training your self to blink at a normal rate - or occasionally taking a break from the CRT - will easily correct this. But so, sadly becoming a plumber will not make my eyes better, but it might make my wallet fatter.So can't you just get new glasses?
The astigmatism that most people have is a "simple" or "monaxial" astigmatism. If you consider the cornea to be like a soft contact lens, flexible and in the shape of a shallow dimple, these astigmatism are caused by squeezing the lens from either side, causing it to barrel or fold along a single axis. Glasses can be made to account for these astigmatism by thinning the lens along a single axis. However with KC, the astigmatism can be extremely complex representing a variety of lumpy or teardrop distortions of the cornea. No lens using traditional materials can correct this situation.Why not be comfortable and use soft contacts?
I wear ( soft ) contacts and I don't have any problems!
Aaaaargh! Once again, with a mild simple astigmatism, it is possible to create soft contacts which perform well. However in KC, the soft contact would just conform to the irregular shape of the cornea, nor providing any improvement in vision. Yes, soft lenses are much more comfortable - but thoroughly ineffective for KC.Well if contacts don't work why wear them?
Aaaaargh! Hello! You're not listening! Soft contacts cannot be used because of the reason above. However RGP ( Rigid Gas Permeable ) lenses are "hard" and won't conform to the irregular surface of the cornea - which also makes them less comfortable. However, they do produce a regular exterior curvature which "smoothes over" the KC irregularities and yields superior vision. The bad part is that your eye was not designed to have a floroacrylate flake stuck on its surface. In addition, many believe that use of RGP lenses may help stabilize the cornea and reduce the chances for scaring which results from stretching of the cornea. So they may also be therapeutic.My [ some relative / friend ] got laser surgery, why don't you?
KC is caused by a thinning of the cornea, in fact it can become so thin that you risk it rupturing, though this is very rare. In addition, the KC cornea is not stable and typically continues to progress over time, sometimes for years, before it stops thinning. Laser surgery requires a healthy cornea and uses years of accumulated statistical info to determine exactly how much material to remove and where to achieve a finished correction. First, the KC cornea is not healthy. Second, there is limited data on show much material would need to be removed to provide a given correction. And third, since the KC cornea is still in a state of flux, the surgery may be a success only to have the cornea progress even further, requiring additional surgeries. In other words, it is an experimental procedure at best and potentially risky.Are there other problems associated with KC?
Photophobia, aka light sensitivity, is a problem for many with KC. I am very sensitive to light, even before wearing contact lenses, and the contacts only exacerbate this. Night / twilight is a very nice time of day. Apical scaring is also a problem.The thinning of the cornea can be so acute as to reduce its thickness by 60%. The cornea can develop scars which can cloud vision even when contacts would otherwise provide a solution.
There are various membranes on the inner surface of the cornea ( exposed to the fluid inside the eye ) which also can be impacted as KC progresses. These membranes regulate the amount of water absorbed by the fibrous stroma which make up the structural part of the cornea. When there is too much water, this cartilaginous material become cloudy. This results in clouded vision, "acute hydrops," which may cloud the cornea so severely that only shapes and colors can be discerned. This will typically resolve itself in a few weeks and is not permanent.
Lessons I've Learned...
First, after diagnosis, find a local expert on KC. This will typically a corneal surgeon who specializes in fixing damaged corneas, performing transplants, etc. This will most likely NOT be the local pusher of laser eye surgery. While it is important to be dealing with someone knowledgable about your problems, but rather they will be able to refer you to their contact fitter - who will become your new best friend.
KC Links - Visit Them Now!
National Keratoconus Foundation
Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study